Introduction
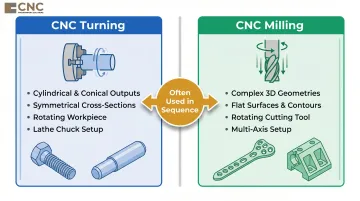
CNC turning rotates a workpiece against a stationary cutting tool to produce cylindrical forms, while milling moves a rotating cutting tool across a fixed workpiece to create complex shapes. Together, they form the backbone of precision medical part manufacturing—an industry valued at USD 1.0 billion in 2024 and projected to reach USD 1.7 billion by 2033.
Medical parts such as bone screws, surgical instrument shafts, and implant components carry zero tolerance for dimensional error. A deviation in a bone screw thread, a burr on a cannula tip, or a rough surface on an implant aren't quality rejects—they're patient safety incidents with direct regulatory and liability consequences.
Medical device recalls hit a 4-year high of 1,048 events in 2024, with a substantial portion traced to manufacturing defects.
While turning and milling are widely referenced in medical manufacturing discussions, the operational difference between them, when each is used, and what determines their precision outcomes is rarely explained in actionable terms. This article covers exactly that — process mechanics, material considerations, tolerances, and where each method fits in a medical production workflow.
Key Takeaways
- CNC turning produces rotationally symmetric parts—shafts, screws, cannulas—by rotating the workpiece against a stationary tool
- CNC milling creates complex 3D geometries like bone plates, housings, and instrument bodies using a rotating cutting tool
- Both processes achieve the micron-level tolerances and biocompatible surface finishes that patient safety demands
- Material choice (titanium, stainless steel, or PEEK) directly determines which process, cutting parameters, and tooling apply
- Precision is driven by CNC programming quality, machine rigidity, fixturing, and post-process finishing
- Part geometry, tolerance requirements, and surface standards determine which process fits—sometimes both are needed in sequence
What Are CNC Turning and Milling in Medical Parts Manufacturing?
CNC Turning
CNC turning is a subtractive process in which the raw workpiece—typically a bar of medical-grade metal or PEEK—spins at controlled speed while a stationary cutting tool removes material to produce cylindrical or conical profiles. Swiss turning is particularly effective for small-diameter bone screws, achieving diameters as small as 0.010" with tolerances to ±0.0002".
Common turned outputs include:
- Threaded fasteners and bone screw blanks
- Cannula bodies and instrument handles
- Tapered shafts, internal bores, and grooved components
The workpiece rotates about its central axis in a lathe chuck or collet while the cutting tool moves radially and axially to shape external diameters, internal bores, threads, tapers, and grooves. This rotational symmetry makes turning ideal for any part where the cross-section remains consistent around a central axis.
CNC Milling
Unlike turning, CNC milling moves a rotating multi-flute cutting tool across a stationary or indexed workpiece along multiple axes, removing material to create flat surfaces, pockets, slots, contours, and complex 3D profiles. Common outputs include bone plates, surgical clamps, implant housings, and instrument jaws.
Multi-axis milling handles screw head drive features (hex, torx, custom geometries) and anatomical contours that lathes cannot efficiently produce.
Three-axis mills generate prismatic features; 4- and 5-axis milling centers allow the cutting tool to approach the workpiece from multiple angles in a single setup, enabling undercuts and compound angles that would otherwise require multiple repositioning steps.
Critical Distinctions from Related Processes
Turning and milling differ fundamentally from:
- Forging: Shapes metal through compressive force to produce rough stock, not finished precision geometry
- Grinding: A finishing operation that refines surfaces, not a primary shaping process
- Additive manufacturing: Builds parts layer-by-layer rather than removing material
Turning and milling are the primary precision shaping steps that take forged or bar stock to near-final geometry. They frequently work in sequence: a turned blank may be transferred to a milling center to add cross-holes, flats, or contoured features. Knowing where one process ends and the other begins directly affects part cost, lead time, and achievable tolerances.
Why Turning and Milling Are Critical for Precision Medical Parts
Tolerance Demands Unique to Medical Manufacturing
Medical parts must routinely hold dimensional tolerances of ±0.001 inches or tighter. In general machining, tolerances of ±0.005" are standard; ±0.001" is considered tight, and ±0.0005" and below are classified as ultra-precision. CNC turning for medical components routinely holds ±0.0002".
Neither ISO 13485:2016 nor FDA 21 CFR Part 820 specify dimensional tolerance values directly—they govern the quality management system framework that requires manufacturers to establish, document, and validate tolerances for each device design.
The FDA recently amended 21 CFR Part 820 to incorporate ISO 13485:2016 by reference, making ISO 13485 certification the baseline expectation for CNC machining suppliers in medical device supply chains.
Medical Applications Demand Specific Process Outcomes
Three process outcomes determine whether a machined part is safe for clinical use:
- Surface biocompatibility: Implant surfaces must meet specific Ra (average roughness) values to prevent tissue irritation. ISO 7206-2:2011 specifies hip joint articulating surfaces shall have an Ra ≤ 2 µm; femoral heads target Ra 0.010–0.015 µm for optimal wear performance.
- Dimensional repeatability: Every part must conform to validated specifications across production runs, with process capability studies (Cpk > 1.33 for critical surfaces) demonstrating statistical control.
- Geometric precision for assembly: Screw-thread engagement in orthopedic implants requires exact thread form and pitch. Misfit causes micromotion at load-bearing joints, leading to implant loosening or catastrophic failure.
What Goes Wrong When Machining Is Executed Poorly
Poor execution in turning or milling causes patient harm:
- Dimensional deviation in bone screw threads prevents proper engagement with bone, reducing fixation strength
- Burrs on cannula tips cause tissue tearing during surgical insertion
- Rough implant surfaces accelerate wear debris generation in articulating joints, triggering inflammatory responses
These aren't just quality rejects—they're patient safety incidents with regulatory and liability consequences.
Regulatory and Operational Drivers
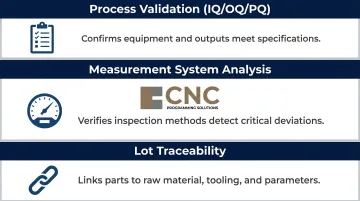
Those consequences drive both the operational choice of CNC machining and its regulatory requirements. ISO 13485-certified environments require documented process control, which CNC machining's programmability directly supports. Manual machining cannot reliably deliver at medical tolerance levels—three capabilities make that clear:
- Process validation (IQ/OQ/PQ): Confirms equipment, processes, and outputs meet specifications before production begins
- Measurement system analysis: Verifies that gauging and inspection methods are accurate enough to detect critical deviations
- Lot traceability: Links every finished part to its raw material, tooling, and process parameters for regulatory audit
How CNC Turning and Milling Work: The End-to-End Process
Conceptual Flow
Raw medical-grade bar stock or forged blank → workholding and fixturing setup → programmed cutting operations (turning and/or milling) → in-process measurement → post-machining finishing → final inspection and documentation.
What "goes into" the process:
- Material selection: Medical-grade stainless steel 316LVM (ASTM F138), titanium Ti-6Al-4V ELI (ASTM F136), cobalt-chrome (ASTM F1537), or PEEK (ASTM F2026-17)
- CNC program: Defined toolpaths, speeds, and feed rates
- Precision fixturing: Holds the workpiece without distortion
Step 1: Material Setup and Fixturing
For turning, bar stock is loaded into a CNC lathe chuck or collet. For milling, the workpiece is clamped in a vise, on a tombstone, or in a custom fixture. In medical machining, workholding must eliminate vibration and flex — any movement during cutting introduces dimensional error that may not be visible until final inspection.
CNC programming then defines the exact sequence of tool movements, depth of cut, spindle speed, and feed rate. Programming quality determines whether the machine executes precise, repeatable cuts or introduces systematic error across every part in a production run.
Step 2: The Cutting Operation
- Turning: The lathe spindle accelerates the workpiece to programmed RPM; the tool removes material in controlled passes. Thread forms, tapers, internal bores, and external diameters are generated with repeatability that manual machining cannot match at medical tolerance levels.
- Milling: A 3-axis mill generates prismatic features. Multi-axis centers allow the cutting tool to approach from multiple angles in a single setup — critical for complex anatomical contours. 5-axis machining delivers 30% cycle time reduction, 60% fewer setups, and 25% increased process accuracy compared to 3-axis operations.

Expert 5-axis CNC programming — the type CNC Programming Solutions provides for medical component work — enables complex 3D contours, undercuts, and deep cavities to be held to specification without repositioning error.
Step 3: Finishing, Inspection, and Compliance
Post-machining finishing:
- Deburring: Vibe deburring removes micro-burrs from edges that could cause tissue injury
- Bead blasting: Creates uniform matte surface texture
- Passivation/anodizing: Enhances corrosion resistance
Each finishing step must be process-controlled and documented for medical device compliance. ASTM F86 mandates cleaning, passivation, and marking protocols specifically for implants, while ASTM B912 defines electropolishing requirements.
In-process and final inspection: CMM (coordinate measuring machine) verification, surface profilometry for Ra measurement, and thread gauging confirm that each part meets drawing specifications before it is logged for traceability. Medical device manufacturers require first article inspection reports, lot traceability records, and certificates of conformance with every shipment per ISO 13485 requirements.
Where Turning and Milling Are Applied Across Medical Device Categories
Process-to-Part Mapping
| Turning | Milling |
|---|---|
| Spinal pedicle screws | Bone plates |
| Cannulated screw bodies | Surgical clamps |
| Rods and fasteners | Endoscopic instrument bodies |
| Pins and miniature shafts | Implant shells and housings |
| Cylindrical implant components | Prosthetic joint components (knee trays, tibial baseplates) |
| Catheter fittings | Pacemaker housings |
| Instrument handles | Complex PEEK components |
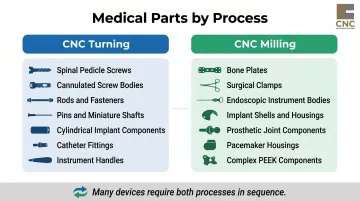
Many finished devices require both processes at different stages. A spinal screw begins as a turned cylindrical blank, then transfers to a milling center for drive feature geometry (hex socket, torx recess).
Medical Device Lifecycle Stages
Machining occurs primarily in:
- OEM production: High-volume manufacturing of commodity medical hardware
- Prototyping and design validation: Machined samples for fit, form, and function testing before regulatory submission
- Custom implants: Low-volume, high-complexity patient-specific devices
Process parameters and programming approach vary across high-volume production runs and custom low-volume work.
Key Factors That Affect Precision Outcomes in Medical Machining
Material Machinability
Titanium Ti-6Al-4V has thermal conductivity of approximately 7.2 W/m-K—heat concentrates at the cutting edge, accelerating tool wear and potentially altering surface integrity. Cutting parameters must be specifically tuned for each medical alloy, unlike general-purpose machining of mild steel.
Sandvik Coromant recommends cutting speeds of 60 m/min for roughing and 180-240 m/min for finishing, with high-pressure coolant systems at 70-100 bar to dissipate heat. Common failure modes include built-up edge (BUE), notching at the cut line, galled workpieces, and chips welding to the cutter.
Tooling Condition and Selection
Worn or incorrect tooling in medical machining doesn't just reduce part quality—it introduces micro-surface defects that become stress risers in implants or crevices that harbor contamination. Research documents that tool wear causes surface cracking, cavities, tearing, grooves, side flow, smearing, and surface burning, with surface topography, microstructure, and residual stress distribution deteriorating as tool wear progresses.
Defined replacement schedules—not reactive changeouts—are what separate acceptable scrap rates from consistent first-article yield.
Machine Rigidity and Thermal Stability
Dimensional drift from machine thermal expansion can move a part out of tolerance during long production runs—often without operator awareness. Parts are designed to be dimensionally correct at 68°F (20°C), but typical shop environments range from 70-75°F. In a 10-meter machine, a 3°F temperature spread produces 0.22 mm of dimensional movement.
Controlling this requires more than ambient air conditioning. High-precision environments target ±1°C stability, with two additional practices:
- Temperature soak: Normalize part and machine at the target temperature for 24 hours before measuring or machining
- Conditioned coolant: Use temperature-regulated cutting fluid to prevent localized thermal spikes at the cut zone
CNC Program Quality and Axis Count
The number of programmable axes determines what geometries can be produced in a single setup. More setups mean more opportunities for positional error. Expert programming for 4- and 5-axis machines eliminates setup-induced variation for complex medical parts.
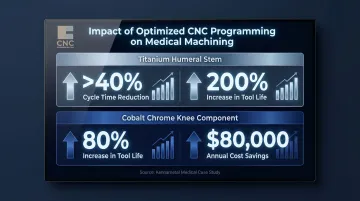
The compounding effect of better programming shows up in real production numbers. A Kennametal case study on optimized medical machining strategies reported:
- Titanium humeral stem: >40% reduction in cycle times, 200% increase in tool life
- Cobalt chrome knee component: 80% increase in tool life, $80,000 in annual cost savings
Regulatory and Quality Constraints
ISO 13485 quality management requirements mean that every process parameter affecting part quality must be documented, validated, and controlled. This makes machining a validated manufacturing process with formal change control—not simply a production operation. Stryker's Supplier Quality Guidebook requires PPAP, FAI, CoC, lot traceability, IQ/OQ/PQ process validation, and MSA (Gage R&R) for critical features.
Common Misconceptions About Turning and Milling for Medical Parts
Tighter Tolerance Always Means Slower Production
Well-optimized CNC programs running on well-maintained machines can hold medical-grade tolerances at production rates. The real bottlenecks are setup, fixturing, and inspection — not the cutting operation itself:
- Setup complexity adds time before the first chip is cut
- Fixturing design determines how many repositions a part needs
- Inspection requirements dictate throughput at the back end
5-axis machining reduces cycle time by 30% and setup count by 60% compared to 3-axis operations for complex geometries, demonstrating that advanced programming actually increases throughput while maintaining precision.
Surface Roughness Equals Surface Cleanliness
A visually smooth machined surface is not automatically biocompatible. Ra (average roughness) must be measured and confirmed against implant or instrument standards. ISO 7206-2 sets a maximum Ra of 2 µm for hip articulating surfaces, but industry practice for femoral heads targets Ra 0.010-0.015 µm, a difference of two orders of magnitude.
Most implant-grade surfaces require additional finishing steps — passivation or electropolishing — before meeting regulatory requirements. Surgical instruments require Ra 0.4-0.8 µm on general surfaces; Ra 0.8 µm is the critical cleanability threshold, as surfaces rougher than this retain biofilm.
Turning and Milling Are Interchangeable
A cylindrical spinal screw must be turned, since milling alone cannot efficiently produce a true cylindrical thread form. Conversely, a complex contoured bone plate cannot be produced on a lathe. Selecting the wrong process increases cost, compromises geometry, and risks tolerance nonconformance.
Conclusion
Turning handles cylindrical precision; milling handles geometric complexity. Together, they address the full range of medical part geometries — from simple fasteners to complex implant bodies.
Knowing which process applies, what controls outcome quality, and how CNC programming ties it all together is practical knowledge with real consequences. Get those decisions right and you produce compliant, patient-safe parts. Get them wrong and you face costly nonconformances.
CNC Programming Solutions provides precision turning, milling, and multi-axis CNC programming services for medical manufacturers. Reach the team at cncsolutions22@gmail.com or 405-714-3714.
Frequently Asked Questions
What is the process of turning?
CNC turning is a subtractive machining process where the workpiece rotates at high speed while a stationary cutting tool removes material, producing precise cylindrical shapes such as shafts, screws, and bores used in medical devices. The process is ideal for rotationally symmetric parts requiring tight tolerances.
What is the difference between CNC turning and CNC milling?
In turning, the workpiece rotates and the tool is stationary (ideal for cylindrical parts); in milling, the cutting tool rotates and traverses the workpiece (ideal for flat surfaces, contours, and complex 3D geometries). Medical parts often require both in sequence.
What materials are most commonly used in CNC machining for medical parts?
Common materials include medical-grade stainless steel 316LVM, titanium Ti-6Al-4V ELI, cobalt-chrome alloys, and PEEK polymer. Each requires specific cutting parameters and tooling due to differences in hardness, thermal properties, and biocompatibility requirements.
What surface finish tolerances are required for precision medical parts?
Hip implant articulating surfaces require Ra ≤ 2 µm per ISO 7206-2, with femoral heads targeting Ra 0.010–0.015 µm; surgical instruments typically fall in the Ra 0.4–0.8 µm range. Post-machining steps like passivation or electropolishing are often required to meet regulatory standards.
How does multi-axis CNC machining improve medical part manufacturing?
4- and 5-axis CNC machining produces complex anatomical geometries in fewer setups, reducing positional error and enabling tighter tolerance control. 5-axis systems deliver 30% cycle time reduction, 60% fewer setups, and 25% greater process accuracy — making them essential for implant shells and surgical instrument bodies.